Xanthelasma
What is xanthelasma?
When the yellowish cholesterol-rich material gets deposited in various parts of a diseased body, xanthelasma is formed. These are lesions which contain deposits that are lipid or fat-rich. This fat accumulates in the macrophage immune cells in the skin and sometimes, even in the layer of fat beneath the skin.
These cutaneous manifestations of lipidosis, in which the lipids cluster within the skin, are associated with hyperlipidemias, both primary and secondary types.
Types of xanthelasma
• Common Xanthelasma
It is demarcated by a yellowish collection of cholesterol that collects under the skin. It is usually found around the eyelids. A xanthoma is a larger and nodular lesion that assumes tumorous proportions and is different from xanthelasma. However, it is often classified as a subtype of xanthelasma.
• Xanthoma Tuberosum
Tuberous Xanthoma is characterized by yellow lesions located over the joints.
• Xanthoma Tendinosum
Tendinous Xanthoma is typically characterized by papules and nodules found in the tendons of the hands, feet, and heels. It is popularly associated with familial hypercholesterolemia.
• Eruptive Xanthoma
Eruptive xanthoma is clinically characterized by small, yellowish-orange to reddish-brown papules that appear all over the body. It is associated with elevated amounts of triglycerides. Xanthoma diabeticorum is associated with severe diabetes
• Xanthoma Planum
Plane xanthoma is a type of xanthelasma that induces macules and plaques to spread over large areas of the body and diffuse
• Palmar Xanthoma
In this condition, yellowish to orange plaques develop on the palms and flexural surfaces of the fingers. These flat macules could also be slightly elevated and often contain a centralized pale area which may be localized or generalized.
They arise in the skin folds, especially the palmar creases. Palmar xanthoma is closely associated with hyperlipoproteinemia type III and type IIA and biliary cirrhosis. It is indicative of hypercholesterolemia.
• Tuberoeruptive Xanthoma
Inflamed red papules and nodules that coalesce form. It is part of the same disease spectrum as eruptive xanthomata.
• Xanthoma Disseminatum
This a rare type of xanthoma, consisting of non-X histiocytosis on flexural surfaces, associated with diabetes insipidus. Hundreds of small yellowish-brown or reddish-brown bumps evenly spread on both sides of the face and trunk. They may particularly affect the armpits and groins. The small bumps may join together to form sheets of thickened skin.
• Xanthoma Verrucous or Histiocytosis
This is associated with papilloma of the oral mucosa and skin, whereby the connective tissue under the epithelium contains histiocytes.
• Diffuse Plane Xanthomatosis
It is associated with an abnormal antibody in the blood called a paraprotein. While lipid levels are normal, about 50% of the conditions have a malignancy of the blood such as multiple myeloma or leukemia. Large flat reddish-yellow plaques over the face, neck, chest, buttocks and in the folds of the skin form.
Detection and Symptoms
Xanthelasma is commonly found on:
• One or both upper eyelids, especially near the nose
• One or both lower eyelids
The lesions appear as a yellow-to-orange patch or bump, ranging in size from 2–30 mm. Xanthelasma is flat-surfaced and has defined borders. Xanthelasma does not usually go away on its own and lesions tend to grow larger and increase in number.
Are You At Risk?
There are several conditions and factors which could make you susceptible to xanthelasma, such as:
• High levels of cholesterol or lipids in your blood; sometimes possible even with normal cholesterol levels
• Middle-aged or older individuals; Ages 15-73 are highly susceptible, with a peak in the 4th and 5th decade
• Female gender over male gender
• Arcus senilis of the cornea
• High blood pressure
• Obesity
• Chain smoking
If any of these conditions and factors pertain to you and you notice symptoms, visit a doctor as soon as possible.
Xanthelasmata can help predict a risk of myocardial infarction, ischemic heart disease, severe atherosclerosis, and death in the general population, independent of well-known cardiovascular risk factors (eg, plasma cholesterol, triglyceride concentrations).
Treatment and Lifestyle Options
Xanthelasma does not go by itself requires medical attention and supervision. If left untreated, it will only spread further.
Apart from surgical methods, an individual’s lifestyle options play a major role. Diet is a major gamechanger. The following measures should be incorporated into your diet:
• A healthy balance of vegetables, salads, cereals, and fish
• The minimization of saturated fats (found in meat, butter, other dairy produce, coconut oil, palm oil)
• Minimised intake of simple and refined sugars (found in soft drinks and confectionery)
• Reduction in calorie intake to lose weight if obese; regular exercise is advocated
Medication has proved to be a very effective alternative to surgery. It can be administered in combination with it as well.
• Statins (HMG CoA reductase inhibitors), such as simvastatin and atorvastatin: Induce reduction in cholesterol production by the liver, thus resulting in lower LDL cholesterol levels, increase in HDL cholesterol and mild reduction in triglycerides. May cause abnormalities if taken in heavy doses.
• Fibrates (bezafibrate): Reduce triglyceride production by the liver, therefore lowering triglycerides and increasing HDL cholesterol levels. May cause gastrointestinal side effects.
• Ezetimibe: If high doses of statins are poorly received or patients are at a high risk, ezetimibe is prescribed. It reduces cholesterol absorption from the gut, lowering total and LDL cholesterol.
• Nicotinic acid: Lowers cholesterol, LDL cholesterol, and triglycerides, and increases HDL cholesterol. Causes flushing if at least one gram is consumed a day for therapeutic purposes. Acipimox is a good alternative.
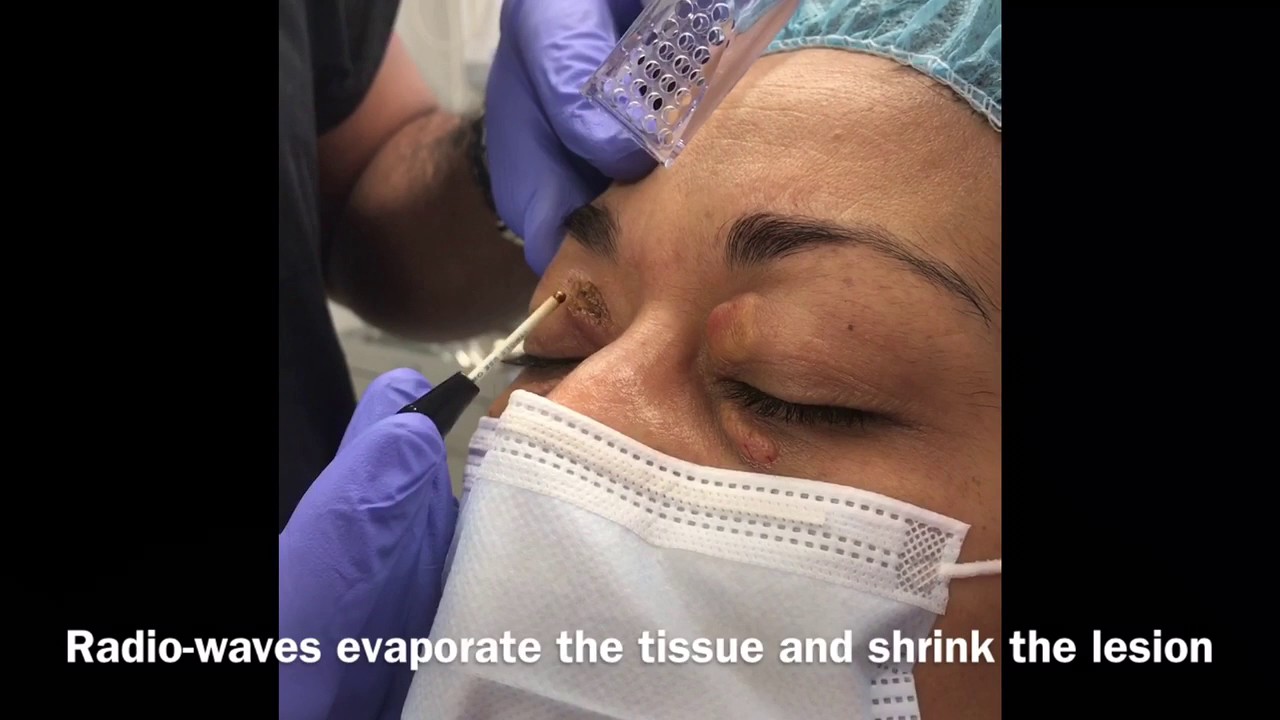
If your xanthelasma does not respond to lipid-lowering medication, the following cosmetic procedures can be undertaken:
• Freezing with liquid nitrogen (cryotherapy)
• Surgical excision
• Laser treatment
• Acetic acid solution to dissolve xanthelasma lesions
• Electric needle treatment (electrodesiccation)
The aforementioned treatments cause scarring and do not prevent new lesions from developing.
It is extremely important that you identify and treat your condition accurately. Clearskin clinics are equipped with safe and state of the art infrastructure to assist you accordingly and provide you with a top-notch treatment.